





Abstract
A healthy diet plays an important role in primary and secondary prevention of cancer. The Mediterranean diet is associated with lower risk of several chronic diseases, including cardiovascular disease, neurodegenerative disease, diabetes, and cancer—especially cancers of the breast and colon. The mechanisms responsible for these effects include reductions in inflammation, oxidative damage, metabolic syndrome, and weight. The Mediterranean diet consists primarily of fish, vegetables, legumes, whole grains, potatoes, fruits, extra virgin olive oil (EVOO), moderate amounts of wine, and small amounts of red meat. It limits processed foods and refined sugar. Achieving this dietary pattern is a simple and attainable goal. Certain food preparation techniques can improve the bioavailability of important nutrients in the Mediterranean diet. Observational and clinical studies show the Mediterranean diet is effective for primary and possibly secondary prevention of cancer.
Introduction
When our patients come to us with the goal of preventing cancer or cancer recurrence, our job is to help them optimize their nutrition, lifestyle, and environment. Food is consumed several times throughout the day, making diet one of the most important factors in the goal of influencing the body's biochemistry and physiology. While specific "super-foods" exist with well-studied phytochemicals, establishing healthy eating patterns is more important to influence overall health. The Mediterranean diet is a simple eating pattern that has gained popularity in recent years, being recommended in the 2015-2020 Dietary Guidelines for Americans. Adherence to a Mediterranean diet is associated with a decrease in chronic diseases such as cardiovascular disease, neurodegenerative disorders such as Alzheimer's and Parkinson's diseases, diabetes mellitus, and cancer.1 This paper reviews the research that shows a correlation between the Mediterranean diet and a decrease in cancer incidence, the mechanisms that may explain the decrease, specific dietary goals to discuss with your patients, how to evaluate adherence to the Mediterranean diet, methods for improving bioavailability of nutrients, and adherence to this dietary pattern.
Cancer prevention
Overall incidence of cancer is lower in Mediterranean countries compared to the United States, United Kingdom, and the Scandinavian countries.2 Large prospective observational studies have linked the Mediterranean diet to this decreased cancer incidence. For example, the MOLI-SANI Project transformed the Molise region of Italy into a “scientific laboratory” of data collection, specifically looking at cardiovascular disease and cancer in relationship to the Mediterranean diet. Other large observational studies, such as the European Prospective Investigation into Cancer and Nutrition (EPIC) and the National Institutes of Health-American Association for Retired Persons (NIH-AARP) Diet and Health study, have subanalyzed the data, looking at the Mediterranean diet, cancer markers, incidence, and mortality. The Greek cohort of the EPIC study (N=25,623) was followed for 7.9 years. Investigators found a 12% reduction in cancer incidence for every 2-point increase in the 10-point Mediterranean diet adherence scale.3 The NIH-AARP Diet and Health study (N=380,296) found a 17% and 12% decreased cancer mortality in men and women following the Mediterranean diet after 5 years of follow-up.4
Breast cancer
Several clinical trials have built upon the data from prospective observational studies. The PREvención con DIeta MEDiterránea (PREDIMED) study is the most well-known, and many analyses have been published from the PREDIMED data. This parallel-group, randomized, multicenter, controlled 5-year trial originally aimed to assess the effects of the Mediterranean diet in primary prevention of cardiovascular disease. A total of 7,447 participants, including 4,282 who were at high risk of cardiovascular events, were randomized to follow one of the following 3 diets: low-fat diet; Mediterranean diet with added EVOO; or Mediterranean diet with added nuts. When compared to a low-fat diet, the risk of combined heart attack, stroke, and death from cardiovascular disease was reduced by 30% in Mediterranean diet + EVOO group and 28% in Mediterranean diet + nuts group.
Cardiovascular risk factors such as blood glucose, blood pressure, low-density lipoprotein (LDL)-cholesterol and C-reactive protein (CRP) were all reduced,5 and the risk of developing type 2 diabetes fell by 52%.6 As an added bonus, in the female cohort they discovered a 68% reduced risk of developing breast cancer in the Mediterranean diet + EVOO group when compared to the low-fat diet group. Each additional 5% of calories from EVOO yielded a hazard ratio of 0.72. An overall 51% reduced risk of breast cancer incidence was found for both Mediterranean diet groups combined. The authors concluded that "this is the first randomized trial finding an effect of a long-term dietary intervention on breast cancer incidence.”7
The NIH-AARP Diet and Health study (N=380,296) found a 17% and 12% decreased cancer mortality in men and women following the Mediterranean diet after 5 years of follow-up.
Now let us look at secondary prevention of breast cancer. Preliminary results of the “SETA PROJECT” were released at the 2016 American Society of Clinical Oncology (ASCO) annual meeting. Of 307 women treated for early-stage breast cancer, 199 were assigned to follow a “normal diet with dietary advice to reduce the occurrence of cancer relapse” (referred to as the Std-Diet) and 109 were assigned to follow the Mediterranean diet. After 3 years of follow-up, 11 cases of recurrence were discovered in the Std-Diet group and no recurrence was found in the Mediterranean diet group.8 Statistical significance was achieved; however, this study is ongoing and we look forward to additional data. Further studies are needed to better evaluate the effect of the Mediterranean diet on secondary prevention such as the DIANA (Diet and Androgens)-5 study that is evaluating the effects of a Mediterranean-macrobiotic diet in women diagnosed with early-stage invasive breast cancer.9
Of note, there is a particular benefit from the Mediterranean diet in the incidence of double- and triple-negative breast cancers. Subanalysis of data from the Grupo Español de Investigación en Cáncer de Mama (EpiGEICAM) study shows a 44% reduced risk of all breast cancer incidence and a 68% reduced risk of development of triple-negative tumors when comparing top vs bottom quartile of Mediterranean diet adherence.10 Data from the EPIC study shows a 7% reduced risk of postmenopausal breast cancer incidence and a 20% reduced risk of estrogen receptor-negative/progesterone receptor-negative breast cancer in high vs low Mediterranean diet adherence.11
Colorectal cancer
The Mediterranean diet is also associated with a reduced risk of colorectal cancer incidence. The Adventist Health Study 2, a prospective North American cohort trial of 77,659 Seventh-day Adventist men and women, compared 4 vegetarian dietary patterns—vegan, lacto-ovo vegetarian, pescovegetarian, and semivegetarian—to a nonvegetarian diet. After 7.3 years of follow-up, the pescovegetarian cohort showed a 43% reduced risk of colorectal cancer incidence when compared with nonvegetarians.12 The Mediterranean diet can be described as primarily pescovegetarian. Data from the EPIC study shows 8% or 11% reduced risk of colorectal cancer incidence,13 depending on the type of Mediterranean diet assessment used, and a 46% reduced risk specifically in the Italian cohort.14 A meta-analysis of 4 prospective cohort and 4 case-control studies of Mediterranean diet and colorectal cancer showed an overall 17% risk reduction.15
Other cancer types
The Mediterranean diet has shown benefit for a reduced risk of many other cancer types. Data from the EPIC study shows a 33% reduced risk of gastric cancer incidence while a meta-analysis shows a 27% reduced risk. A 42% reduced risk of liver cancer incidence was found in 2 studies. The NIH-AARP Diet and Health study showed a 56% reduced risk of squamous cell carcinoma of the esophagus.15
Mechanisms of Action
Metabolic syndrome
Growing data support the association of metabolic syndrome and its components with cancer development and cancer-related mortality. A systemic review and meta-analysis shows a strong link between cancer and metabolic syndrome, with a 61% increased incidence for endometrial, 58% for pancreatic, 56% for postmenopausal breast, and 52% for rectal cancers in women with metabolic syndrome.16
An intervention study of 180 participants with metabolic syndrome were equally divided to follow the Mediterranean diet or the Prudent diet (control). After 2 years of follow-up, resolution of metabolic syndrome was seen in 50 vs 12 patients, respectively. Compared to controls, those following the Mediterranean diet increased their intake of monounsaturated fat, polyunsaturated fat, fiber, fruit, vegetables, nuts, whole grains, and olive oil, with a lower ratio of omega-6/3. The Mediterranean diet group had significantly reduced hs-CRP, interleukin (IL)-7, IL-18, and insulin resistance, and improved endothelial function.17
Data from the PREDIMED trial showed a 35% increased resolution of metabolic syndrome in the Mediterranean diet with EVOO group and 28% in the Mediterranean diet with nuts group when compared to the control diet group. They found significant decreases in central obesity and high fasting glucose. They concluded that "the abundance of healthy, nutrient-dense foods that make up the plant-based Mediterranean diet predicts its bioactivity and potential to beneficially influence metabolic pathways that lead to MetS [metabolic syndrome] and T2 DM [type 2 diabetes mellitus] as well as other chronic conditions.”18
Weight loss
Extra adipose tissue can have deleterious effects on the body that affect the metabolic milieu and raise the risk of cancer incidence and progression, such as producing hormone and growth factors and increasing inflammatory markers. For many of our patients seeking primary and secondary cancer prevention, achieving a healthy weight is an important goal. The PREDIMED study did not restrict calories or encourage physical activity, yet a 0.43 kg weight loss was found in the Mediterranean diet with EVOO group and a 0.94 cm decreased waist circumference was found in the Mediterranean diet with nuts group.19 In an intervention trial comparing low-fat, Mediterranean, and low-carbohydrate diets in 322 moderately obese participants, the Mediterranean diet group lost 4.4 kg, compared to 2.9 kg in the low-fat group, and 4.7 kg in the low-carbohydrate group after 2 years of follow-up.20
Inflammation
Inflammation is recognized as a major factor in the pathology of many chronic diseases, including cardiovascular disease, diabetes mellitus, Alzheimer's disease, and, of course, cancer. Diet plays an important role in either increasing or decreasing the inflammatory response, depending on dietary choices. Acute inflammation can occur during the postprandial state as a result of hyperlipidemia and hyperglycemia. This can be exacerbated by advanced glycation end products (AGEs) and mitigated by antioxidants in the diet. Healthy dietary patterns are associated with lower circulating concentrations of inflammatory markers. Whole grains, vegetables, fruits, and fish, all important components of the Mediterranean diet, are all associated with lower inflammation.21
A 2010 systematic literature review found that the Mediterranean diet is associated with lower circulating markers of inflammation.22 The MOLI-SANI study evaluated for low-grade inflammation based on CRP, leukocyte, platelet counts, and granulocyte/lymphocyte ratio, and decreased levels of these inflammatory markers were detected in relation to the Mediterranean diet. The granulocyte/lymphocyte ratio is of particular interest as it is not only a marker of inflammation, but is also associated with a poorer prognosis in cancer acting as an independent predictor of tumor growth, metastasis, and progression.23
Antioxidant action
Free radical damage can have direct effects on DNA. Regular consumption of antioxidants in the diet improves total antioxidant capacity, thereby protecting the cell. Oxidative damage can also have secondary effects by increasing the inflammatory response and affecting genetic expression. In an extensive review of the link between oxidative stress, inflammation, and cancer, the authors conclude that "oxidative stress can activate NF-κB [nuclear factor kappa light chain enhancer of activated B cells], AP-1, p53, HIF-1α [hypoxia-inducible factor 1-alpha], PPAR-γ [peroxisome proliferator-activated receptor gamma], β-catenin/Wnt, and Nrf2 leading to expression of over 500 different genes, including growth factors, inflammatory cytokines, chemokines, cell cycle regulatory molecules, and anti-inflammatory molecules leading to transformation of a normal cell to tumor cell, tumor cell survival, proliferation, chemoresistance, radioresistance, invasion, angiogenesis and stem cell survival.”24
The Mediterranean diet is abundant in antioxidant-rich fruits and vegetables and is linked to increased total antioxidant capacity and decreased oxidative load. Data from the PREDIMED study shows that blood levels of Ferric Reducing Antioxidant Potential (FRAP) at baseline and after 1 year of dietary interventions showed increases in both the Mediterranean diet with EVOO group (FRAP 72.0 μmol/L) and the Mediterranean diet with nuts (48.9 μmol/L) group, but not with the low-fat diet group. Similar results were found for total radical-trapping antioxidant parameters (TRAPs).25 PREDIMED data also found decreased in vivo LDL oxidation in both Mediterranean diet groups.26
Data shows a link between increased antioxidant intake, specifically from the polyphenol content of the Mediterranean diet, and decreases in low-grade inflammation. Polyphenol content of the Mediterranean diet was negatively associated with low-grade inflammation based on decreased levels of CRP, leukocyte, platelet counts, and granulocyte/lymphocyte ratios,27 as well as decreased VCAM-1 and ICAM-1 (cell adhesion molecules), IL-6, tumor necrosis factor (TNF)-α and monocyte chemoattractant protein(MCP) -1.28
Understanding the Mediterranean Diet
The Mediterranean diet is a dietary pattern that is rich in fish, vegetables, legumes, whole grains, fruits, potatoes, EVOO, and moderate amounts of wine. It is a dietary pattern with reduced intake of meat, poultry, and full-fat dairy products. In my experience of living in a Mediterranean country, the diet is simple, made-from-scratch, and follows the seasons. However, the validated questionnaires that measure adherence to the Mediterranean diet do not take these factors into account. Despite this omission, we continue to see benefit from this dietary pattern even outside of the Mediterranean region.29
Assessing adherence to the Mediterranean diet
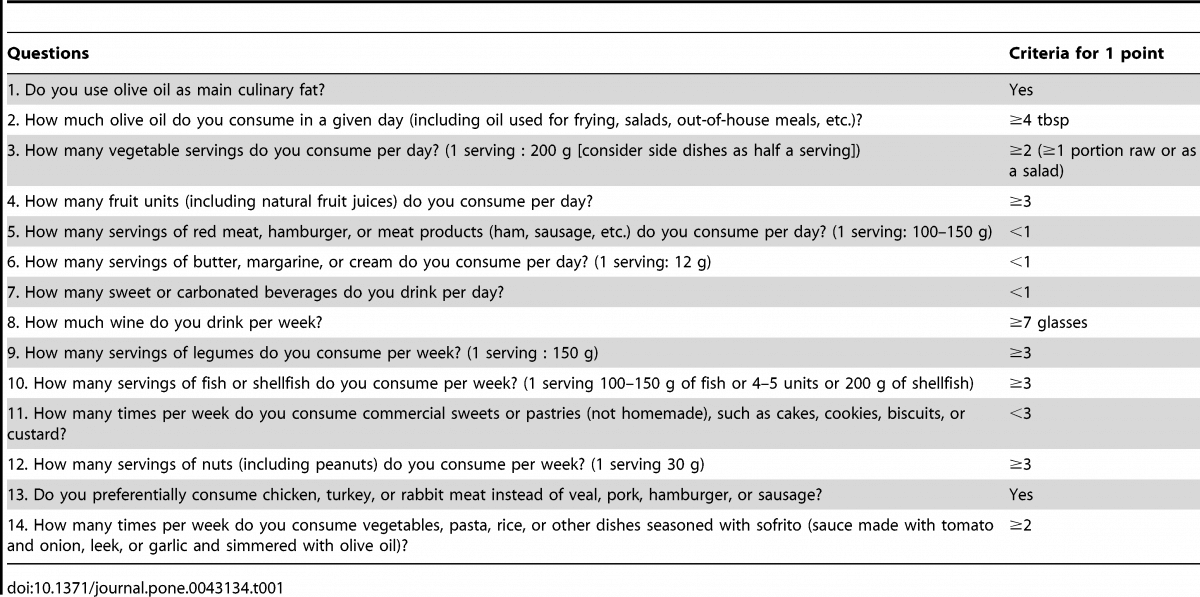
The validated MedDietScore has been used in many observational studies including the PREDIMED study. It awards more points for above-average consumption of the following foods: fish, vegetables, legumes, whole grains, fruits, potatoes, and olive oil, and fewer points for above-average consumption of meat, poultry, and full-fat dairy products. Points for wine consumption are assigned as follows (listed per day): 1-2 glasses (5 points); 2 glasses (4 points); 3 glasses (3 points); 4 glasses (2 points); 5 glasses OR no wine (0 points). This questionnaire contains 137 questions, and the answers must be entered into a software program to determine amounts eaten.30
A 14-question survey was used alongside the MedDietScore in the PREDIMED study and found to be an accurate assessment of adherence to the Mediterranean diet. The questionnaire has also been validated in independent studies.31 Compared to other assessments, this questionnaire (Figure) is more economical to administer and has the advantage of allowing immediate feedback to participants.
Figure
PLoS One. 2012;7(8):e43134.
Recommendations for following the Mediterranean diet
Tied into the 14-question survey listed above are the recommendations that were given to the women in the PREDIMED trial: 4 or more tablespoons of olive oil per day (EVOO for the women in the Mediterranean diet + EVOO group); 3 or more 30 g servings of tree nuts and peanuts per week (or daily for the women in the Mediterranean diet + nuts group); 3 or more servings of fresh fruits per day; 2 or more servings of vegetables per day; 3 or more servings of fish (especially fatty fish) per week; 3 or more servings of legumes per week; 2 or more servings of Sofrito per week (a sauce made with tomatoes and onions, often including garlic and aromatic herbs, slowly simmered in olive oil similar to an Italian pasta sauce); white meat instead of red meat; 7 or more glasses of wine per week consumed with meals (optionally, only for habitual drinkers). The following foods were discouraged: soda drinks (less than 1 drink per day); commercial baked goods (less than 3 servings per week); spread fats (less than 1 serving per day); and red and processed meats (less than 1 serving per day).32
The diet also recommended eliminating or limiting the consumption of cream, butter, margarine, cold meat, pate, duck, carbonated and/or sugared beverages, pastries, industrial bakery products (such as cakes, doughnuts, or cookies), industrial desserts (puddings, custard), french fries or potato chips, and out-of-home pre-cooked cakes and sweets. Ad libitum consumption was allowed for the following food items: nuts (raw and unsalted), eggs, fish (recommended for daily intake), seafood, low-fat cheese, chocolate (only dark chocolate, with more than 50% cocoa), and whole-grain cereals. Limited consumption (≤1 serving per week) was advised for cured ham, red meat (after removing all visible fat), and cured or fatty cheeses. In addition to these recommendations, the dietitians insisted that two main meals per day should be eaten seated at a table, lasting more than 20 minutes.33
These 14 primary goals are attainable to the average patient and have been associated with significant benefit in the large PREDIMED clinical trial. These are goals that I focus upon during my patient visits with the exception that I work toward limiting the discouraged foods to a less frequent schedule.
Nutrient Bioavailability
The manner in which food is prepared can affect its nutrient content, formation of harmful substances, and bioavailability of phytochemicals. Some nutrients can be lost during the cooking process; on the other hand, some nutrients become more bioavailable when cooked. Salad is a simple way to incorporate raw vegetables into the diet and is consumed very frequently in Mediterranean countries. Salads also have the advantage of incorporating antioxidant-rich ingredients in the dressing such as EVOO, lemon juice and aromatic herbs. Other tips for improving bioavailability of nutrients through proper food preparation are discussed below.
Extra virgin olive oil
Extra virgin olive oil consists mainly of oleic acid and contains tocopherols, carotenoids, and as many as 36 distinct polyphenols. These polyphenols have been well-studied and are thought to have antiaging and cancer-fighting effects. For example, oleuropein and hydroxytyrosol, both polyphenols found in EVOO, were shown to decrease angiogenesis via downregulation of COX-2 expression, matrix metallopeptidase 9 (MMP-9) protein release, NF-κB activation, and reduction of intracellular reactive oxygen species (ROS) levels. Other EVOO polyphenols were found to stimulate apoptosis via B-cell lymphoma 2 (Bcl-2), phosphatidylinositol-3-kinase (PI3K)/AKT (also called protein kinase B) signaling, June-NH2 kinase (JNK), p53, p21, Bax, and cytochrome C.34
Olive oil consists mainly of monounsaturated fats and is not appropriate for cooking at high temperatures. Fortunately, cooking at low and medium heat is common practice in Mediterranean countries. While frying significantly decreases the amounts of hydroxytyrosol, other polyphenols are more stable. In one study, heating EVOO to 180°C (356°F) did not affect the reduced postprandial inflammatory response noted in obese subjects.35 Raw EVOO is also consumed abundantly in the Mediterranean diet, with EVOO added to salads as well as drizzled generously over cooked foods such as soups, stews, fish, and vegetables.
Extra virgin olive oil is obtained completely by mechanical means from the first pressing of the olives. Olive oil that is not extra virgin is obtained from the remains of the first (or subsequent) pressing and is extracted with the use of solvents. The amount of polyphenols in non-EVOO is virtually absent, and it is important to make this distinction clear to our patients.
Food fraud is unfortunately prevalent in the olive oil industry. Up to 69% of imported "extra virgin" samples fail to meet international standards.36 Buyers can look for certification from various organizations such as the California Olive Oil Council (COOC), Extra Virgin Alliance (EVA), or UNAPROL, a respected Italian olive growers association. Good-quality EVOO should be dark yellow or green in color and should have a slightly bitter flavor, which is from the polyphenol oleuropein.
Eating olives is another method of including EVOO into the diet. Olives have a high polyphenol content and are generally eaten raw. Olives should be purchased with the pits as the pitting process decreases hydroxytyrosol by approximately half. Kalamata olives have the highest hydroxytyrosol content, followed by Spanish-style green and then Greek-style naturally black olives.37 California-style black olives should be avoided as most of the hydroxytyrosol is removed and acrylamide (a carcinogen) is produced during the oxidation process that converts the green olives to black.38 If olives are included as a substantial source of polyphenols, one may consider rinsing them to decrease the salt content.
Tomatoes and carotenoid foods
Tomatoes and other carotenoid-containing foods are a good example of foods that have improved bioavailability when processed and cooked. Chopping, blending, and cooking help release carotenoids from the food matrix. Cooking tomatoes in fat promotes absorption of the carotenoids across the intestinal wall by incorporating the carotenoids into lipid micelles. Compared to foods cooked with other fats, carotenoid-rich foods cooked in olive oil have improved bioavailability of carotenoids because nutrients from the olive oil are absorbed into the food. The amount of fat, however, is even more important than the type of fat. It is recommended that carotenoid-rich foods be cooked with sufficient fat to promote absorption,39 approximately 3 to 5 g per meal.40 I have learned from many chefs that a tomato-based pasta sauce should have a thin layer of fat at the top, and that the sauce is not ready until that fat turns red.
Cruciferous vegetables
Cruciferous vegetables are good examples of foods that have improved bioavailability of phytochemicals when eaten raw, but they are infrequently eaten raw in the Mediterranean diet due to their strong flavor. Cruciferous vegetables contain polyphenols, carotenoids, tocopherols, vitamin C, and glucosinolates (GSL). Glucosinolates are dependent on the enzyme myrosinase to be converted into bioactive products such as sulforaphane. This enzyme is deactivated at higher temperatures during the cooking process. Eating raw cruciferous vegetables, such as arugula, alongside a cooked-cruciferous meal can provide these enzymes. Adding raw cruciferous vegetables restores up to 100% of sulforaphane formation in blanched-and-frozen broccoli.41
Glucosinolates in vegetables are lost when they leach into the cooking liquid. Soups and stews, the most common way of consuming cruciferous vegetables in the Mediterranean diet, retain the liquid, and thus the nutrients. Soups and stews also have the advantage of having a mix of flavors with sweeter vegetables, such a carrots or fennel, balancing the bitter flavor of the cruciferous vegetables.
Alliums
Alliums contain flavonoids and organo-sulfur compounds. They are another example of foods that have improved bioavailability of phytochemicals when eaten raw but are infrequently eaten raw in the Mediterranean diet. Organo-sulfur phytochemicals require enzymes for activation, such as alliinase, which is required for the production of allicin. These enzymes are housed within the cell, making cell disruption through crushing (garlic) or chopping/grating (onion) necessary for this process to begin. The process also requires time once the enzymes are activated. When these foods are brought to higher temperatures during the cooking process, the enzymes are deactivated40 and so the crushing, chopping and/or grating should happen approximately 20 minutes before they are cooked. I recommend that patients crush, chop, and/or grate the garlic and onions when they first enter the kitchen to begin cooking. Once they have gathered, cleaned, and prepared the other ingredients to be cooked, enough time should have elapsed before the alliums hit the pan.
Nuts
Nuts are an important part of the Mediterranean diet and are rich in unsaturated fats, protein, arginine, fiber, minerals, tocopherols, folate, magnesium, and calcium. The highest concentration of phenolic antioxidants is found in the skin. Removing the skin reduces the total antioxidant capacity of hazelnuts by 36%, walnuts by 90%, and pistachios by 55%.40 It is recommended, therefore, to purchase nuts with the skin intact. Other fat-soluble antioxidants are present in the kernel, though, and nut consumption even without the skin should be encouraged.
The women in the PREDIMED study were encouraged to eat raw nuts. Nuts contain primarily monounsaturated and polyunsaturated fatty acids, which could be affected by higher temperatures. Clinical studies, however, show that the cardiovascular benefits of eating nuts were similar when raw or roasted nuts were consumed.42 I have found that compliance improves significantly when I recommend raw and roasted nuts instead of exclusively raw nuts.
Improving Adherence
Helping patients successfully implement dietary changes can prove to be one of the more difficult tasks of any practitioner. Participants in the PREDIMED study met with dietitians quarterly for 5 years, yet challenges with adherence were still evident.43 While dietary counseling and recipe handouts can be helpful, learning the flow in the kitchen is the ultimate goal. This includes knowing which ingredients to have on hand, how to prepare dishes using a variety of seasonal ingredients, and how leftovers from one meal can be transformed into the next. The Med-Food Anticancer Program is an Italian state-run program with the goal of promoting the Mediterranean diet and physical activity in the adult population. The program offers cooking classes and has published data that shows improved adherence to the Mediterranean diet is associated with resultant improvement in anthropometric, dietary, and metabolic parameters.44
Conclusion
The Mediterranean diet is a dietary pattern that has been practiced for generations in the Mediterranean region. It is a diet abundant in fresh ingredients prepared in a simple manner. The Mediterranean diet is linked to decreased incidence of many chronic diseases, with robust data supporting its correlation with reduction of cancer, specifically of the breast and colon. This effect may be due to reduction of metabolic syndrome, weight, inflammation, or oxidative damage. The recommendations for following the Mediterranean diet can be summarized in 14 achievable goals that have shown benefit in a large clinical trial. Extra virgin olive oil is an important component of the Mediterranean diet. Certain nutrients abundant in the Mediterranean diet can have improved bioavailability through various cooking techniques. Evidence suggests that the Mediterranean diet is an effective dietary pattern for primary, and possibly secondary, prevention of cancer.
