





Reference
Chei CL, Loh JK, Soh A, Yuan JM, Koh WP. Coffee, tea, caffeine, and risk of hypertension: The Singapore Chinese Health Study. Eur J Nutr. 2017 Mar 1. doi: 10.1007/s00394-017-1412-4. [Epub ahead of print]
Design
Population-based prospective cohort
Study Objective
To determine the relationship between coffee and tea consumption and hypertension.
Participants
Data were collected from the Singapore Chinese Health Study, which is a population-based prospective cohort that recruited 63,257 Chinese participants, aged 45 to 74 years, who resided in Singapore from 1993 to 1998. Information on coffee and tea consumption and other lifestyle factors was collected at baseline. Self-reported physician-diagnosed hypertension was assessed during 2 follow-up interviews (1999-2004, 2006-2010).
Study Medication and Dosage
At recruitment, in-person interviews were used to collect information on demographics, height, weight, lifetime tobacco use, current physical activity, sleep duration, and medical history. A detailed questionnaire was used to collect information on food consumption, including alcohol, coffee, and tea. These questionnaires included intake frequency of standard servings of coffee, black tea, and green tea using 9 categories: never or hardly ever; 1 to 3 times a month; once a week; 2 to 3 times a week; 4 to 6 times a week; once a day; 2 to 3 times a day; 4 to 5 times a day; and 6 or more times a day.
Outcome Measures
Cox proportional hazards models were used to estimate the hazard ratios (HRs) and 95% confidence intervals (CIs) for risk of hypertension associated with coffee, black tea, green tea, and caffeine intake.
Key Findings
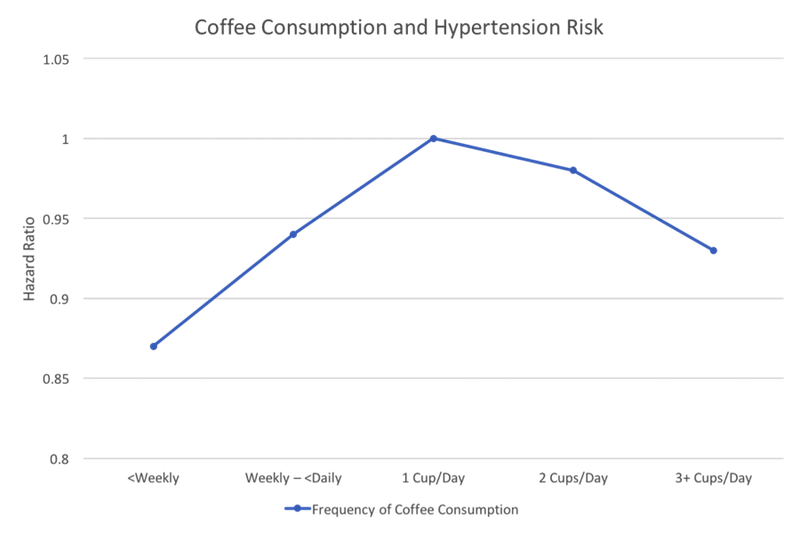
Over a mean follow-up of 9.5 years, 13,658 cases of hypertension were diagnosed among the cohort. The hypertensive patients were more likely to be women, never-smokers, and non-drinkers of alcohol. They were also older, less educated, had higher body mass index (BMI), and were more physically active. Results from multivariable analysis revealed an inverse U-shaped association between coffee intake and risk of hypertension. Compared to drinking 1 cup per day, drinking coffee less frequently was associated with a reduction in risk of hypertension. Similarly, the risk was also decreased in those who drank more than 2 cups per day. In the multivariable analysis, compared to those who drank 1 cup per day, the HRs of incident hypertension were as follows: 0.94 (95% CI: 0.88-1.00) for weekly to <daily (less than 1 cup per day); 0.87 (95% CI: 0.83-0.91) for those who drank less than weekly; 0.98 (95% CI: 0.94-1.02) for those who drank 2 cups per day; and 0.93 (95% CI: 0.86-1.00) for those who drank ≥3 cups per day.
Think of how this might translate into clinical practice: In speaking to a patient with mild hypertension who admits to drinking 1 cup of coffee each morning, your advice based on this study should be, 'Either stop drinking coffee or start drinking a whole lot more.'
The association between coffee intake and incidence of hypertension did not vary significantly between men and women (P<0.5 for all interactions). See Figure.
Figure
Participants who drank black tea daily had slightly increased risk (9%) compared to those who consumed black tea less than weekly (HR: 1.09; 95% CI:1.03-1.15). Similar results were observed for green tea (HR: 1.06; 95% CI: 1.00-1.11). However, these associations were not statistically significant when adjusted for caffeine content.
There was a statistically significant positive association between caffeine intake and risk of hypertension; compared with <50 mg/day caffeine intake, all 4 higher categories of caffeine intake had statistically significant increase in risk of hypertension, but without a clear dose-dependent trend.
After adjusting for coffee (such that the caffeine intake was from other sources), the stepwise dose-response relationship between caffeine intake and hypertension risk became more apparent. Compared to the lowest intake (<50 mg/d), the multivariable HRs for 50 to <100, 100 to <200, 200 to <300, ≥300 mg per day were 1.07 (95% CI: 1.00–1.15), 1.10 (95% CI: 1.02–1.18), 1.08 (95% CI: 0.98–1.19), and 1.16 (95% CI: 1.04–1.31; P for trend=0.02) respectively.
Practice Implications
Participants who drank less than 1 cup of coffee per week or more than 2 cups of coffee per day had a significant reduction in risk of hypertension compared to those who drank 1 cup per day.
Think of how this might translate into clinical practice: In speaking to a patient with mild hypertension who admits to drinking 1 cup of coffee each morning, your advice based on this study should be, “Either stop drinking coffee or start drinking a whole lot more.”
As odd as this sounds, we should take these results seriously. They are consistent with conclusions from a 2011 dose–response meta-analysis of 5 cohort studies that also suggested an inverse U-shaped or J-shaped association between coffee and the risk of hypertension.1 In that meta-analysis, risk of hypertension increased with coffee consumption and peaked at 3 cups per day, but the risk decreased at higher levels of coffee consumption. These current Chei findings are also similar to several prospective studies that found a nonlinear association among cohorts of European men and women,2,3 US nurses,4 and other health professionals.5 Moderate coffee drinkers (1-3 cups/day) were found to have the highest risk of hypertension compared to light drinkers who drank less than 1 cup per day and heavy drinkers who drank more than 3 cups per day. A 2007 Dutch study reported a similar inverse J-shaped association in which hypertension risk was reduced for those who drank less than 1 cup of coffee per day and those who drank more than 3 cups per day compared to those who drank 1 to 3 cups per day.6 These current findings continue to confirm what at first glance is a peculiar phenomenon, the inverted U-shaped curve of dose response.
It comes as no surprise that caffeine raises blood pressure; it does so through “mechanisms that include sympathetic over-activation, antagonism of adenosine receptors, increasing norepinephrine release via direct effects on the adrenal medulla, direct renal effects, and activation of the renin–angiotensin system.”7 Yet coffee appears to have other attributes so that high doses attenuate the caffeine effect.
Coffee is a rich source of potassium, and 5 cups per day supplies about 26% of daily intake of potassium.8 Potassium promotes vascular smooth muscle relaxation and endothelium-dependent vasodilation, increases endothelial nitric oxide production, and has a blood pressure-lowering effect in animals and humans.9 Chlorogenic acid, a major polyphenol in coffee, may also account for the blood pressure-lowering action of coffee. Chlorogenic acid has been shown to reduce blood pressure and improve endothelial dysfunction in hypertensive rats10 and in mildly hypertensive humans.11
Thus what may be going on is that moderate doses of coffee, in the 1 to 2 cup per day range, raise risk of hypertension because of the influence of caffeine. At higher doses these other chemicals may counter the caffeine influence and lower blood pressure.
If coffee’s effect on blood pressure is actually dose-specific, this may explain the inconsistencies seen in other epidemiologic studies that looked for associations between coffee consumption and cardiovascular disease.12
By the way, although technically a cup of coffee is usually defined as 150 mL of liquid or about 5 fluid ounces, rather than the 8 ounces that normally constitute a cup, in this current study, a cup of coffee was defined as 237 mL, a nearly full 8-ounce cup.
U-shaped dose-response curves are being reported with greater frequency in the literature, and we must assume that this form of response is more common than originally understood. As a result it is likely that our dietary and nutritional recommendations may become more complex in the future as we realize that effects may change with changes in dose size. While more may not always be better, in the case of coffee it just might be.
